

By Josephine Shenouda, DrPH, MS, Emily Barrett, Ph.D., Amy L. Davidow, Ph.D., Kate Sidwell, BA, Cara Lescott, BA, William Halperin, MD, DrPH, MPH, Vincent M. B. Silenzio, MD, MPH, Walter Zahorodny, Ph.D. and editorial Lisa Ackerman
A new study sharing important findings on intellectual disability (ID) in autism and disparities in underserved communities has been released. You can find their full paper in the reference section of this blog (1.)
First, I want to thank the study authors for their work: Prevalence and Disparities in the Detection of Autism Without Intellectual Disability. It is valuable work sharing important findings in how we look at autism.
This blog contains two parts:
Part one: key message findings from the study authors
Part two: an editorial opinion from TACA’s Executive Director on how the autism community could benefit from these findings
Part one is the key findings from this new study. Authors include: Josephine Shenouda, DrPH, MS, Emily Barrett, Ph.D., Amy L. Davidow, Ph.D., Kate Sidwell, BA, Cara Lescott, BA, William Halperin, MD, DrPH, MPH, Vincent M. B. Silenzio, MD, MPH, Walter Zahorodny, Ph.D.
Bottom line up front:
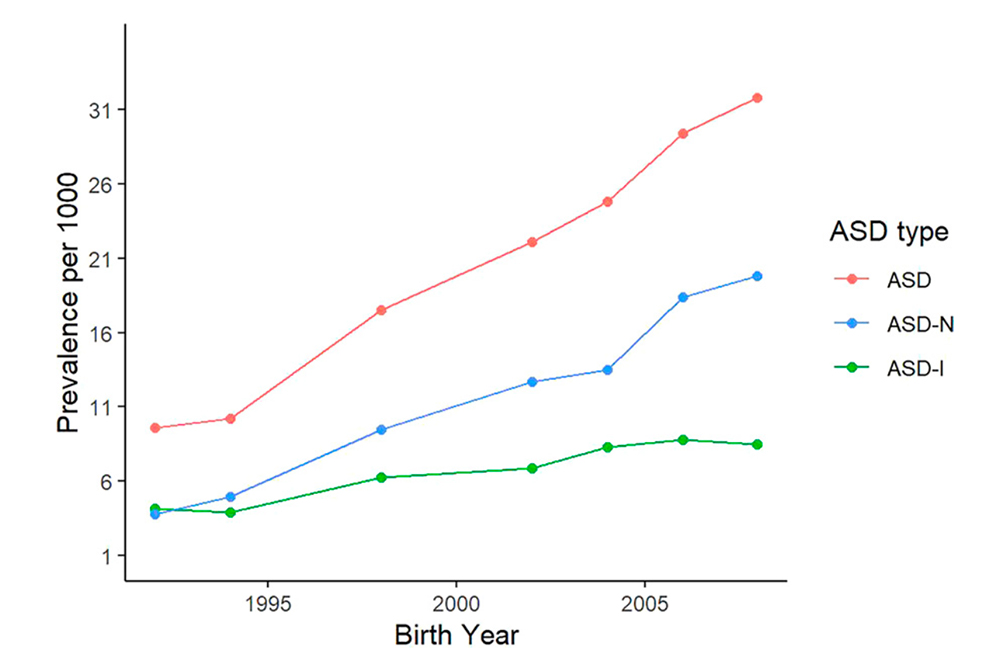
The expression of autism spectrum disorder (ASD) may have changed over time. Past studies have shown that many children identified with autism also have an intellectual disability. Our findings show that 2 in 3 children identified with autism do not have ID. Autism rates have increased from 2000-2016 in the Metropolitan New York-New Jersey region; however, the increase was not equally distributed. While we observed a 2-fold increase in prevalence estimates for autism with co-occurring ID, estimates increased 5-fold for autism without co-occurring ID. Our findings also reveal disparities in identification of autism without co-occurring ID among underserved populations. Non-Hispanic Black children and children residing in socially disadvantaged regions were less likely to be identified with autism without co-occurring ID compared to Non-Hispanic White children and children residing in economically affluent regions, respectively.
Key Findings:
- From 2000-2016, autism prevalence estimates increased 3-fold from approximately 1% in 2000 to 3% in 2016 in the New York-New Jersey Metropolitan Area.
- Children identified with autism without ID grew at a faster rate (5-fold increase) compared to children identified with autism and ID (2-fold increase).
- Approximately 2-in-3 children identified with autism do not have ID.
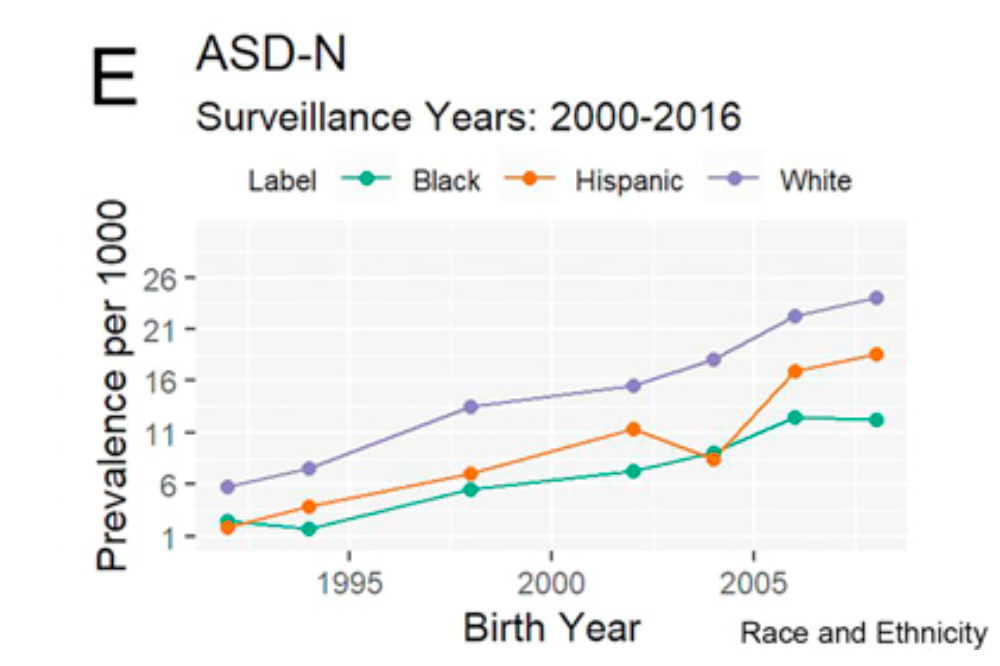
- Non-Hispanic Black children were 30% less likely to be identified with autism without ID compared to Non-Hispanic White children.

- Children residing in affluent areas were 80% more likely to be identified with autism without ID compared to children residing in underserved regions.
- Male to female ratio among children with autism and ID was slightly lower than among children with autism and no ID.
Key Messages:
Even in a metropolitan area with abundant resources and services, disparities in autism identification among historically disadvantaged populations remain. Innovative strategies are needed to improve identification of autism without ID disability among these populations.
Autism rates in the New York-New Jersey Metropolitan area likely reflect rates in other metro areas. While the study shows a 3-fold increase overall in autism rates, we expect autism estimates to continue to rise as disparities in identification are addressed.
Universal autism screening before 36 months with improved linkage to care is needed to identify children with autism early, and also likely to have the greatest effect on children from underserved communities
Study Data:
This study used cross-sectional data from an active surveillance system developed by the CDC called Autism and Developmental Disabilities Monitoring (ADDM) Network. New Jersey has been part of the ADDM Network since its inception back in 2000 and has completed 7 cycles of surveillance tracking autism prevalence among 8-year-olds in the same region, using the same case definition and methodology.
Part Two shares an editorial opinion on this new study. My goal is to share thoughts and possible takeaways to support the autism community. Again, I am grateful to the study authors for this work. They continue to publish important insights into the complex and multifaceted autism spectrum diagnosis.
In this study there are two key points:
- ID is not as common as once thought. Only 1/3 of those diagnosed with autism have ID. That is a significant departure from what has been shared previously.
- After over 22 years of service with TACA it is clear, autism has the same problem as other chronic health conditions. Affluent families have easier access to screening and care. The study sited: children residing in affluent areas were 80% more likely to be identified with ASD without ID compared to children in underserved areas. There is a large divide of families in underserved communities. Addressing these communities must become a priority.
This study helps us understand the changes in previous findings and how we can change our view and the way we look at autism. In my opinion, there are three important takeaways to include from this insightful study:
- Pediatricians are in an ideal position to address diagnostic inequalities in underserved communities. When suspected, pediatricians can refer patients to be assessed so they can receive early intervention and medical attention unique to each individual’s needs. There is room for improvement (2.)
- Researchers concluded that there is a need to address health disparities in the identification of ASD through the expansion of screening programs and improved connection to ASD healthcare to improve outcomes for individuals.
- Once again investing in early intervention and presumed competence in individuals diagnosed with autism with therapies and treatments is a worthwhile endeavor for future outcomes.
- Diagnosis clarity should be a goal going forward. Autism is too broad of a label. For those with ID profound autism and treatment standards would be helpful in driving appropriate treatments.
Autism and its rapid increase in prevalence require innovative solutions, funding, and support. Studies like this one demonstrate that what we once thought, no longer applies when it comes to ID. In addition, every child in every community living with autism needs the same access to treatment and care. We must do better. Now that we know, we need to care, and to act.

DSM – 6 is needed now. RPM and S2C are changing everything about how those with Autism will be raised, treated, educated. socialized and employed. It is imperative that there is an about-face in education and treatment methods for autism. They are demonstrating, and they are literally TELLING us, they are stuck inside bodies that are not easily controlled, but that their intelligence is viewable and able to be demonstrated. Behaviors are their only communication so squelching and repressing behaviors is not humane treatment. The movie, http://www.spellers.io, and many books written by those with Autism, are the beginning of this, the Autism Revolution.
Hello Here is my feedback. My daughter has autism traits but can learn anything it just depends on how to connect with her methodologies for learning. i have designed a few books which meet her learning style for reading, listening and speaking(responding in context. They work for her but that’s because the book was designed to enable her to connect with the learning methodology she uses. I had to do this because if not my child’s development would have been undermined.
Children inflicted with Autism are not being enabled towards individual methods of learning, they are being trapped and institutionalised, here is why? 1. The materials used in therapies, teaching, training are corporate produced and highly restrictive and make the wrong assumptions about how a subject or activity steering development should be given. In fact for many children the opposite outcome to what is claimed is being done. The providers claim the materials are flexible for differentiated teaching/training, that is simply not true.(Delaying and stymieing development) ( Creating a long term type of customer?) 2. Therapists and other types of training/teaching staff are being trained to use those restrictive corporate methods and materials. (Delaying and stymieing development) ( Creating a long term type of customer?) 3. The corporations involved donate/influence certificated courses and in return they can influence the training content for therapists etc. They ensure that the only widely available resources are produced by them. 4. This point has to be said. Every issue has a cause and for far too long the causation factor has been misrepresented to hide the real cause. If we cannot pinpoint the real cause we cannot stop what is happening to children. Expect millions more children around the planet to be afflicted. Autism has become a global industry and the unfortunate customers are a huge source of corporate profit. This makes all of us guilty of ignoring finding out the real cause of the harming and neutralising it.
Sincerely
Richard Haberkost
Dare to be Wise. Never accept being taught, not to think.
[image: Change Is How We Grow Dark Comment Symbols]
DSM 6 is needed. Am Speech Language Hearing Association needs to help address non speaking individuals and recognize other communication abilities.
Many want to explain away autism. It needs attention, better labels, to drive treatments and therapies.
It’s not the language load. Evaluations of our children all all fine-motor heavy—speech and writing. Imagine I tied your hands behind your back and put tape over your mouth and asked you questions. This is essentially how schools are testing our children. We know speech (the articulation of sound) and language (ascribing meaning to those sounds) are in different lobes of the brain. The connecting cable is impaired…along with sensory and motor.