


By Richard Frye, MD, PhD
Phoenix Children’s Hospital, Phoenix AZ
Autism Spectrum Disorder (ASD) is an enigma to even the most educated scientists, doctors, educators, psychologists, and others. Despite decades of research, we are not much closer to knowing what causes ASD and have limited evidence on how best to treat it. Meanwhile the numbers continue to rise. So why does it seem that medicine is so inept when it comes to ASD? A quick consideration of history might be helpful.
Autism is New
Autism is a rather new disorder in the history of medicine. We can find descriptions of most medical disorders in the medical literature from several hundred or even thousands of years ago. Indeed, the Greeks described many medical disorders, even though they weren’t completely accurate about what caused them or even how the body worked. However, autism was only identified in the last century. Specifically, two physicians independently described a series of patients with symptoms that would come to be known as autism in the 1940s.1
It was not until 1980 that autism was defined as its own disorder in the Diagnostic and Statistical Manual of Mental Disorders, Third Edition (DSM-III )1 So, not only is autism a new disorder in the history of medicine, it is also a new disorder in the history of defining psychiatric disorders. To add even more confusion, the exact constellation of symptoms used to define autism, as well as the diagnostic categories, have changed as the DSM has been updated. In the most current version of the DSM, the DSM-5, autism is considered a true spectrum, and is named Autism Spectrum Disorder (ASD), without the subtypes defined in the previous version of the DSM. The current version of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), which provides the diagnostic codes used in medical billing and treatment, also contributes to the confusion by continuing to list several of the old subtypes, such as Asperger’s Syndrome, which have been essentially abandoned by the DSM-5.
Early theories of the causes of ASD focused on psychological and genetic causes, leading to a high concentration of behavioral and genetic research, which continues despite limited practical results. In fact, the research community has only recently begun to embrace abnormalities in the body physiology (the way the body works).2 Most importantly, the high concentration of genetic research has limited the search for treatments. Most genetic disorders are thought not to be treatable, since we cannot change our genes. Luckily, research into other physiological abnormalities of the body that might be amenable to treatment, such as disorders of mitochondrial function; folate and oxidative stress metabolism; and the contribution of immune dysfunction are gaining traction, albeit slowly.2 Research into environmental causes2,3 and strategies for prevention also are gaining some ground.
Measuring Autism’s Prevalence is Even Newer
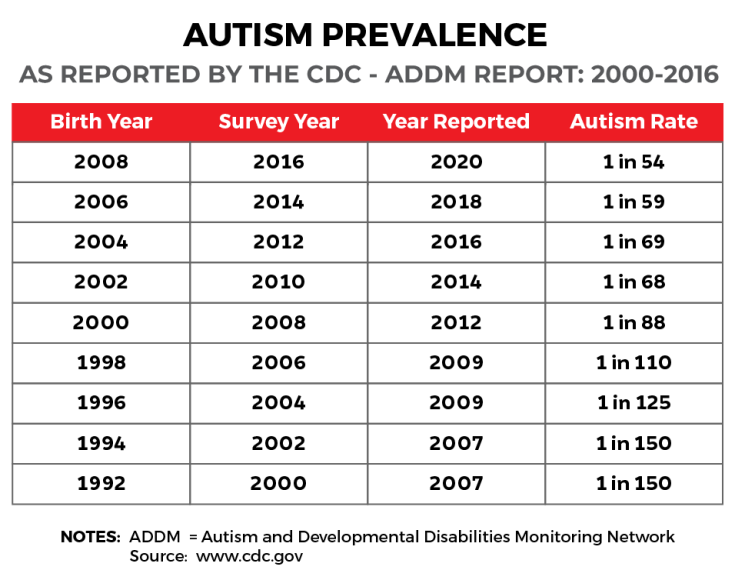
Because of autism’s status as a new disorder with unknown etiology, it was not until this century that the Centers for Disease Control and Prevention (CDC) carefully examined its prevalence by creating the Autism and Developmental Disabilities Monitoring Network (ADDM) in 2000. The ADDM has grown to 11 centers that monitor the prevalence of ASD, based on the review of records from community-based medical and educational service providers in their states. Since the network’s inception, the prevalence estimate was based on review of the records of 8-year-old children. Since 2010, a subset of the network (six sites) has also monitored the prevalence of ASD in 4-year-old children. The ADDM publishes Surveillance Summaries about every two years in the CDC’s Morbidity and Mortality Weekly Report. Importantly, these summaries provide numbers calculated four years prior to their publication – and therefore are four years behind current trends.
Over the first decade of this century, the ADDM found rate increases from 1 in 150 children for the year 20004 to 1 in 68 for the year 2010.5 Despite this striking, almost threefold increase over 10 years, the vigorous debate around ASD focused on whether the increase was real, or whether it could be attributed to better diagnosis and awareness of the disorder. Meanwhile, as the arguments go on, the numbers continue to climb.
The Most Recent Estimate
The most recent ADDM report was released just recently. What did it tell us?
First, the numbers rose again. The recent report, which provides prevalence numbers for 2016, estimates that 1 in 54 8-year-old children is diagnosed with ASD – almost 2% of children!6 This represents a 10% increase over the previous report two years ago and a 175% increase since the beginning of monitoring in 2000. The ADDM report also found that the new DSM-5 diagnostic criteria reduce the diagnosis of ASD by 2%, compared to the diagnostic criteria from the DSM-IV-TR . Thus, the prevalence continues to increase even as the diagnostic criteria identify fewer children with ASD.

For 4-year-old children, it is estimated that 1 in 64 is diagnosed with ASD in 2016,7 an increase from 1 in 75 in 2010, the first year 4-year-old children were monitored.8 So you may ask, why are the prevalence rates lower in 4-year-old children than in 8-year-old children? Is it because children are developing ASD at older ages? Absolutely not. One of other major findings of these studies is that despite an intense effort by the medical community to increase early diagnosis and screening for ASD, there was no change in the average age of diagnosis. Children are still not being identified early in life, which is crucial, since the one thing we know from research is that early identification and intervention is one of the only things we can do to ensure optimal outcomes.
The reports are also mention several other sources of ASD population prevalence, including the National Survey of Children’s Health and the National Health Interview Survey, which both estimate the prevalence of ASD in 3- to 17-year-old children to be 1 in 40, suggesting that 2.5% of children have ASD! The CDC has introduced an interactive tool that shows ASD prevalence estimates from multiple sources. (https://www.cdc.gov/ncbddd/autism/data/index.html). What is most striking and worrisome about the comparisons on this website is that the organizations that provide services for ASD (Medicaid and Special Education Child Count) report prevalence rates at about half of those reported by the ADDM network and the National Survey of Children’s Health.
Where do we go from here?
Over the past decade there has been a push for earlier detection and intervention. However, innovative tools for screening and diagnosis are only starting to be developed. Screening tools provided to primary doctors are still not being used as recommended, and even when children are identified there are long waiting lists to receive evaluations. At Phoenix Children’s Hospital, we, like others, are training community-based primary care pediatricians to become qualified to use tools to diagnose children on the front lines. However, reimbursement is poor and only the most heroic and energetic doctors can integrate such practices into their office. New technology has allowed alternative methods for evaluating children by having psychologists review videos recorded by parents, thereby streamlining the processes. However, research shows that gold-standard diagnostic tools, which are based on behavioral observations, are only stable down to 24 months of age. Even when children are identified early, only a handful of states in the US can provide them the services they need, and medical insurance is not helpful in many cases for funding the behavioral and educational therapies that are known to .
The lifetime cost of caring for a person with ASD is estimated at about $3.6 million, and that total lifetime costs since 1990 for society has been $7 trillion, a number that will grow to $15 trillion in the next 10 years if the prevalence continues to increase.9 Thus, we need an effort the size and speed of the Manhattan Project to find causes and treatments for ASD. We were able to build the atomic bomb in three years in order to cause historical destruction; can’t we turn our efforts toward curing one of the most historic disorders of our lifetime? Efforts of the US are great when they need to be, and this is definitely the time they are needed. We just spent 2 trillion dollars stimulating the economy – you would think we could have found a few crumbs in there for autism research and treatment.
References
- Frye RE. Social Skills Deficits in Autism Spectrum Disorder: Potential Biological Origins and Progress in Developing Therapeutic Agents. CNS Drugs. 2018 Aug;32(8):713-734.
- Rossignol DA, Frye RE. A review of research trends in physiological abnormalities in autism spectrum disorders: immune dysregulation, inflammation, oxidative stress, mitochondrial dysfunction and environmental toxicant exposures. Mol Psychiatry. 2012 Apr;17(4):389-401.
- Rossignol DA, Genuis SJ, Frye RE. Environmental toxicants and autism spectrum disorders: a systematic review. Transl Psychiatry. 2014 Feb 11;4:e360.
- Autism and Developmental Disabilities Monitoring Network Surveillance Year 2000 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders–autism and developmental disabilities monitoring network, six sites, United States, 2000. MMWR Surveill Summ. 2007 Feb 9;56(1):1-11.
- Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years – autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014 Mar 28;63(2):1-21.
- Maenner MJ, Shaw KA, Baio J; EdS1, Washington A, Patrick M, DiRienzo M, Christensen DL, Wiggins LD, Pettygrove S, Andrews JG, Lopez M, Hudson A, Baroud T, Schwenk Y, White T, Rosenberg CR, Lee LC, Harrington RA, Huston M, Hewitt A; PhD-7, Esler A, Hall-Lande J, Poynter JN, Hallas-Muchow L, Constantino JN, Fitzgerald RT, Zahorodny W, Shenouda J, Daniels JL, Warren Z, Vehorn A, Salinas A, Durkin MS, Dietz PM. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years – Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill Summ. 2020 Mar 27;69(4):1-12.
- Shaw KA, Maenner MJ, Baio J; EdS1, Washington A, Christensen DL, Wiggins LD, Pettygrove S, Andrews JG, White T, Rosenberg CR, Constantino JN, Fitzgerald RT, Zahorodny W, Shenouda J, Daniels JL, Salinas A, Durkin MS, Dietz PM. Early Identification of Autism Spectrum Disorder Among Children Aged 4 Years – Early Autism and Developmental Disabilities Monitoring Network, Six Sites, United States, 2016. MMWR Surveill Summ. 2020 Mar 27;69(3):1-11.
- Christensen DL, Maenner MJ, Bilder D, Constantino JN, Daniels J, Durkin MS, Fitzgerald RT, Kurzius-Spencer M, Pettygrove SD, Robinson C, Shenouda J, White T, Zahorodny W, Pazol K, Dietz P. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 4 Years – Early Autism and Developmental Disabilities Monitoring Network, Seven Sites, United States, 2010, 2012, and 2014. MMWR Surveill Summ. 2019 Apr 12;68(2):1-19.
- Cakir, J, Frye, RE, Walker, SJ. The lifetime social cost of autism: 1990–2029. Research in Autism Spectrum Disorders. 2020; 72: 101502

Thank you, it’s very interesting. Concerning the folate link, I started a page on Cerebral Folate Deficiency in Wikipedia (in Russian and English), and I hope further studies will clarify whether there is a definite causal association with autism.